Anterior Cruciate Ligament Reconstruction Surgery
Knee Ligament Injuries
The major ligaments that contribute to knee stability are the Anterior Cruciate Ligament (ACL), Posterior Cruciate Ligament (PCL), Medial Collateral Ligament (MCL) and Posterolateral corner (PLC) which itself consists of multiple ligaments including the Lateral Collateral Ligament (LCL) and popliteus. Any one or combination of these ligaments can be damaged- commonly from sports injuries but also from significant falls/impacts to the leg or motor vehicle accidents.
Management of Knee Ligament Injuries?
Management of these knee ligament injuries are individualised depending on factors including injury factors (severity and pattern of ligament injury), patient factors (age, previous injuries or surgeries, pre-existing arthritis) as well as sporting and functional goals. Non-operative treatment with physiotherapy, muscle strengthening and temporary bracing may lead to the desired goals in certain situations such as isolated PCL or MCL injuries. In cases of associated meniscal injuries, multiple-ligament involvement, ACL or PLC injuries, surgery is usually recommended.
What is ACL Reconstruction?
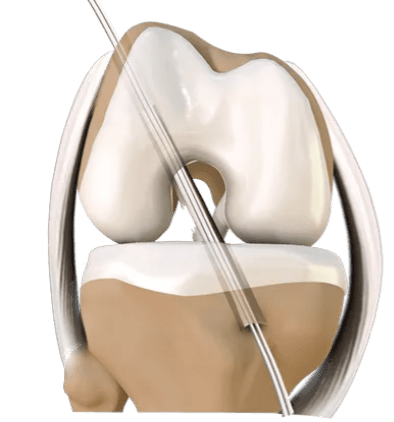
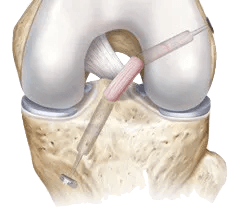
The Anterior Cruciate Ligament is one of the major stabilising ligaments in the knee. It is a strong rope-like structure located in the centre of the knee running from the femur to the tibia. When this ligament tears unfortunately it doesn’t heal and often leads to the feeling of instability in the knee- particularly with pivoting and side to side movements.
ACL reconstruction is a commonly performed surgical procedure and with recent advances in arthroscopic surgery can now be performed with minimal incisions and low complication rates. Surgery can be performed as a day procedure or an overnight stay. Most ACL surgeries are reconstructions. This involves replacing the damaged tissue with a substitute tissue called a graft, as the native torn ACL has minimal capacity to heal itself (even after surgical repair). The most commonly used grafts involve use of tissue from the patient (autografts)- usually utilising either a hamstring tendon or a section of the patellar tendon. Tissue from donor patients (allografts) can also be used in certain circumstances. There are pros and cons for each option which your surgeon will discuss with you at the time of your consultation.
Prehabilitation and rehabilitation
Physiotherapy is an integral part of the treatment and is recommended to start as early as possible. Pre-operative physiotherapy is important in preparing the knee for surgery. The early aim is to regain range of motion, reduce swelling and achieve full weight-bearing.
Postoperative rehabilitation will be supervised by a physiotherapist and is an essential part of your recovery. It involves a graduated increased in knee activity and exercises over time and upon meeting functional goals, with the end result to get you back to your desired sport, work, leisure or day to day activities.
